Indications: In combination with ulnar nerve block and radial nerve block, all operations on the Hand Special Contraindications: none Landmarks: Palmaris longus tendon1 Puncture site3: Directly lateral to the palmaris longus tendon Insertion of needle: Introduce the cannula vertical to the skin 0,5-1 cm deep (if there is a strong resistance to injection, retract 2 mm) Dosage: 2 ml 1 % lignocaine or prilocaine or 0,5% bupivacaine
Di laman ini kita akan membincangkan satu lagi jenis penyakit bawaan nyamuk yang kadang kala berlaku di Malaysia. Soalan-soalan dibawah ini adalah soalan yang kerap ditanya oleh sesiapa sahaja yang ingin mengetahui mengenai penyakit ini – Demam Chikungunya….Jadi manfaatkannya…
Apakah itu demam chikungunya?
Virus Chikungunya pertama kali dijumpai di Tanzania, Afrika Timur tahun 1952. Tidak hairanlah apabila namanya pun berasal dari bahasa Swahili. Ertinya adalah yang berubah bentuk atau bongkok. Postur badan pesakitnya memang kebanyakan membongkok akibat kesakitan yang teramat di persendian tangan dan kaki. Virus ini termasuk keluarga Togaviridae, Genus alphavirus, dan dibawa oleh Nyamuk Aedes Aegypti.
Sejauh manakah kekerapan berlakunya penyakit ini?
Sejurus penemuan virus ini di Afrika, epidemik berlaku di Filipina (1954, 1956 dan 1968), Indonesia (1973), Thailand, Kemboja, Vietnam, India, Myanmar, Sri Lanka dan Indonesia. Sejak tahun 2003, terdapat beberapa kes berlaku di kepulauan Lautan Pasifik termasuk Madagascar, Comoros, Mauritius dan La Reunion, dengan jumlah kes yang meningkat ketara selepas bencana tsunami pada Disember 2004.
Memetik laporan AFP, sebanyak 148 kematian (secara langsung dan tidak langsung) telah dilaporkan sehingga Mac lalu di La Reunion dengan satu per tiga daripada penduduknya yang berjumlah 777,000 jatuh sakit disebabkan oleh virus ini. Selain insiden yang mula dikesan penularannya sejak 1 April lalu di Bagan Panchor, Pantai Remis, Perak, negara pernah dilaporkan dua kali menghadapi penyakit ini iaitu pada tahun 1999 di Pelabuhan Klang melibatkan 27 mangsa (majoritinya pendatang asing). Kes chikungunya yang pertama sekali di Malaysia pernah dilaporkan sekitar tahun 1960-an.
Bagaimanakah virus ini merebak?
Penyakit chikungunya boleh dikatakan ‘bersaudara’ dengan penyakit demam denggi dan demam denggi berdarah kerana dibawa oleh pembawa yang sama iaitu nyamuk aedes sama ada aegypti mahupun albopictus. Masa inkubasi virus ini ialah dua sampai empat hari, sementara manifestasinya tiga sampai sepuluh hari.
Bezanya, jika virus denggi menyerang pembuluh darah, virus chikungunya menyerang sendi dan tulang.
Nyamuk aedes lazimnya akan menggigit seseorang yang telah dijangkiti oleh virus chikungunya dan memindahkan darah berkenaan kepada seorang mangsa lain yang sihat.
Apakah tanda-tanda orang yang telah terkena virus ini?
Simptom-simptom penyakit chikungunya secara klinikalnya sangat mirip kepada demam denggi. Ia lazimnya dimulai dengan demam tinggi secara mendadak sehingga mencecah 39 celsius. Simptom lain termasuklah kesejukan, menggigil, ruam pada kaki, tangan dan badan, kurang selera makan, perut meragam, sakit kepala, mata merah, sedikit fotofobia (sensitif kepada cahaya), loya dan muntah.
Gejala paling biasa adalah sakit sendi (artritis atau atralgia) terutamanya di hujung jari, pergelangan tangan dan buku lali, atau rasa ngilu pada tulang.Jangkitan chikungunya juga mungkin tidak menunjukkan sebarang gejala (asimptomatik) atau menyebabkan kesakitan yang teruk dan gejala yang berpanjangan.
Mujurlah, penyakit chikungunya tidak menyebabkan kematian seperti denggi berdarah. Ia dikategorikan sebagai penyakit yang boleh sembuh dengan sendirinya. Kalaupun berlaku kematian, ia adalah dalam jumlah yang kecil.
Jadi, kenapa perlu bimbang?
Dalam tempoh seminggu, pesakit berada dalam keadaan kesakitan yang akut (sangat teruk) sehingga tidak boleh bergerak atau berjalan (kelumpuhan sementara) sekali gus menjejaskan kualiti hidupnya. Pesakit biasanya akan mengalami demam selama lima hingga tujuh hari sebelum beransur-ansur hilang. Ia bagaimanapun boleh berulang kembali. Jangan lupa, chikungunya sekeluarga dengan denggi berdarah. Tambahan pula, gejalanya hampir serupa. Ia juga boleh melemahkan sistem imun tubuh, menyebabkan badan mudah dijangkiti oleh penyakit-penyakit lain
Adakah seseorang itu boleh dijangkiti virus chikungunya beberapa kali dalam hidupnya?
Tidak. Mana-mana individu yang pernah dijangkiti virus ini secara semula jadinya akan membina daya ketahanan yang bertahan lama.
Bagaimanapun, sesetengah daripada mereka mungkin mengalami sakit sendi yang berpanjangan dari beberapa minggu ke bulan lamanya dan berulang-ulang dalam tempoh yang agak lama, disebabkan oleh reaksi sendi dan bukannya jangkitan virus.
Adakah seseorang yang telah dijangkiti boleh menularkan penyakit chikungunya kepada orang lain pula?
Tidak. Seseorang yang telah dijangkiti tidak boleh menyebarkan penyakitnya itu secara langsung kepada orang lain. Proses penularan hanya berlaku menerusi nyamuk pembawa.
Adakah ia boleh dirawat?
Seperti demam denggi berdarah, belum terdapat ubat-ubatan mahupun vaksin bagi mencegah penyakit chikungunya. Rawatan sedia ada yang diberikan hanya bersifat simptomatik (sokongan, mengikut gejala bagi mengurangkan kesakitan).
Misalnya, pesakit diberikan ubat demam atau penahan sakit. Pesakit dinasihatkan banyakkan minum air dan istirehat yang cukup.
Pesakit akan diasingkan dan seboleh-bolehnya elakkan daripada kemungkinan terdedah kepada digigit nyamuk, sebagai salah satu usaha mencegah penyebaran virus itu kepada orang lain.
Bagaimana hendak mencegah virus ini dari terus menjangkiti orang lain?
Memandangkan tiada rawatan aktif mahupun rawatan pencegahan penyakit chikungunya, satu satunya cara mengelakkan jangkitan adalah dengan mengurangkan pendedahan terhadap jangkitan nyamuk ke tahap maksimum. Ini termasuklah memusnahkan sarang pembiakan larva bagi menghentikan rantaian kitar hidup dan penularannya. Antara pelbagai pilihan lain bagi melindungi diri anda daripada gigitan nyamuk termasuklah:
* Tidur menggunakan kelambu
* Pakai baju berlengan panjang atau berseluar panjang terutamanya ketika berada di luar
rumah pada waktu senja bagi mengelakkan pendedahan langsung kulit terhadap gigitan
nyamuk aedes
* Pasang penghadang nyamuk pada tingkap
* Pasangkan ubat nyamuk lingkaran, elektrik atau menggunakan semburan racun serangga
* Biarkan pengudaraan berlaku sama ada dengan kipas angin atau alat penghawa dingin
* Sapu krim repelen serangga yang disahkan selamat pada kulit dan pakaian.
Indications: In combination with ulnar nerve block and median nerve block, all operations on the hand Special Contraindications: none Landmarks: Pulsation of the radial a.1 Puncture site2: About 1 cm lateral to the pulsation of the radial a. Insertion of needle: Parallel to the wrist subcutaneously Dosage: 5 ml 1% lignocaine or prilocaine or 0,25% bupivacaine
Indications: In combination with the 3 in 1-block, all operations on the lower limb Special Contraindications: none Landmarks:: Posterior superior iliac spine1, greater trochanter2 Puncture site: 3 cm below middle of line joining 1 & 2 Insertion of needle: Introduce the needle vertical to the skin 6-8 cm deep Dosage: 20-30 ml 1 % lignocaine or prilocaine or 0,5% bupivacaine
II. Anterior Sciatic Nerve Block
Landmarks: Inguinal ligament1, greater trochanter2 Puncture site: At the point of intersection of a line from the junction of the middle third and the medial third of the inguinal ligament with a line parallel to the inguinal ligament at the greater trochanter level Insertion of Needle: Slight lateral direction to contact the femur, retract the needle to the subcutaneous area and correct the direction until the needle slides off the femur, then push forward approx. 5 mm Dosage: 10-20 ml 1% lignocaine or prilocaine or 0,5% bupivacaine
3 in 1-block
The lumbar plexus is "sandwiched" (Winnie) between the psoas major m. and the quadratus lumborum m. and enveloped by their sheaths Local anaesthetic runs up from the injection site and blocks the femoral n., the lat. cut. n. of thigh and the obturator n. Indications: In combination with sciatic nerve block, all operations on the lower limb Special Contraindications: none Landmarks: Inguinal ligament2, femoral a.1 Puncture site: Below the inguinal ligament, 1-1,5 cm lateral from the femoral a. Insertion of Needle: In slightly cranial direction Dosage: 25—30 ml 1 % lignocaine or prilocaine or 0,5% bupivacaine
Chikungunya fever, is a viral illness that is spread by the bite of infected mosquitoes. The disease resembles dengue fever, and is characterized by severe, sometimes persistent, joint pain (arthritis), as well as fever and rash. It is rarely life-threatening. Nevertheless widespread occurrence of diseases causes substantial morbidity and economic loss
Epidemiology
Epidemics of fever, rash and arthritis, resembling Chikungunya fever have been recorded as early as 1824 in India and elsewhere. However, the virus was first isolated between 1952-1953 from both man and mosquitoes during an epidemic of fever that was considered clinically indistinguishable from dengue, in the Tanzania.
Chikungunya fever displays interesting epidemiological profiles: major epidemics appear and disappear cyclically, usually with an inter-epidemic period of 7-8 years and sometimes as long as 20 years. After a long period of absence, outbreaks of CHIK fevers have appeared in Indonesia in 1999.
Chikungunya in Asia (1960-1982)
Between 1960 and 1982, outbreaks of Chikungunya fever were reported from Africa and Asia. In Asia, virus strains have been isolated in Bangkok in 1960s; various parts of India including Vellore, Calcutta and Maharastha in 1964; in Sri Lanka in 1969; Vietnam in 1975; Myanmar in 1975 and Indonesia in 1982.
Recent occurrences of chikungunya fever
After an interval of more than 20 years, chikungunya fever has been reported from several countries including India, and various Indian Ocean islands including Comoros, Mauritius, Reunion and Seychelles.
Chikungunya fever in India
Till 10 October 2006, 151 districts of eight states/provinces of India have been affected by chikungunya fever. The affected states are Andhra Pradesh, Andaman & Nicobar Islands, Tamil Nadu, Karnataka, Maharashtra, Gujarat, Madhya Pradesh, Kerala and Delhi.
More than 1.25 million cases have been reported from the country with 752,245 cases from Karnataka and 258,998 from Maharashtra provinces. In some areas attack rates have reached up to 45%.
Chikungunya and dengue fevers
The clinical manifestations of chikungunya fever have to be distinguished from dengue fever. Co-occurrence of both fevers has been recently observed in Maharashtra state of India thus highlighting the importance of strong clinical suspicion and efficient laboratory support.
Laboratory Investigation
The clinical manifestations of chikungunya fever resemble those of dengue fever. Laboratory diagnosis is critical to establish the cause of diagnosis and initiate specific public health response.
Treatment, prevention and control
Treatment
Chikungunya fever is not a life threatening infection. Symptomatic treatment for mitigating pain and fever using anti-inflammatory drugs along with rest usually suffices. While recovery from chikungunya is the expected outcome, convalescence can be prolonged (up to a year or more), and persistent joint pain may require analgesic (pain medication) and long-term anti-inflammatory therapy.
Prevention and control
No vaccine is available against this virus infection. Prevention is entirely dependent upon taking steps to avoid mosquito bites and elimination of mosquito breeding sites.
To avoid mosquito bites:
Wear full sleeve clothes and long dresses to cover the limbs;
Use mosquito coils, repellents and electric vapour mats during the daytime;
Use mosquito nets – to protect babies, old people and others, who may rest during the day. The effectiveness of such nets can be improved by treating them with permethrin (pyrethroid insecticide). Curtains (cloth or bamboo) can also be treated with insecticide and hung at windows or doorways, to repel or kill mosquitoes.
Mosquitoes become infected when they bite people who are sick with chikungunya. Mosquito nets and mosquito nets and mosquito coils will effectively prevent mosquitoes from biting sick people.
To prevent mosquito breeding
The Aedes mosquitoes that transmit chikungunya breed in a wide variety of manmade containers which are common around human dwellings. These containers collect rainwater, and include discarded tires, flowerpots, old oil drums, animal water troughs, water storage vessels, and plastic food containers. These breeding sites can be eliminated by
Draining water from coolers, tanks, barrels, drums and buckets, etc.;
Emptying coolers when not in use;
Removing from the house all objects, e.g. plant saucers, etc. which have water collected in them
Cooperating with the public health authorities in anti-mosquito measures.
Indications: Completion of incomplete peridural anaesthesia or sciatic nerve block, diagnostic, therapeutic and operative interventions in the area of innervation, especially fractures of the lateral part of the ankle and ruptures of the lateral ligament. Special Contraindications: none Landmarks: Head of fibula1, biceps femoris tendon2 Puncture site3: Immediately posterior to fibula, 2 cm below head Insertion of needle: Introduce the needle vertical to the skin approx. 1 cm deep Dosage: 5 ml 1 % lignocaine or prilocaine or 0,5% bupivacaine
Indications: Completion of incomplete peridural anaesthesia or sciatic nerve block; in combination with common peroneal and saphenous nerve block: operations in the area of lower leg and foot Special Contraindications: none Landmarks: Internal and external epicondyles of femur, medial and lateral gastrocnemius m. Puncture site: In the middle of the line connecting the lateral and medial epicondyles of femur. Insertion of needle: Introduce the needle vertical to the skin 1,5-3 cm deep Dosage: 5-10 ml 1% prilocaine or 0,5% bupivacaine
Indications: Completion of incomplete femoral nerve block, in combination with tibial and fibular nerve block: operations of lower leg and foot Special Contraindications: none Landmarks: Medial condyle of tibia, pes anserinus, tibial tuberosity 1, gastrocnemius m. Puncture site: At the medial part of the tibial tuberosity Insertion of needle: S.c. infiltration from the medial part of the tibial tuberosity to the gastrocnemius m. Dosage: 5-10 ml 1% lignocaine or prilocaine or 0,5% bupivacaine
Landmarks: Medial malleolus1, tibial a.2 Puncture sites: On both sides of the tibial a. Insertion of needle: Introduce the needle vertical to the skin 0,5-2 cm deep Dosage: 2-3 ml of 1% prilocaine or 0,5% bupivacaine
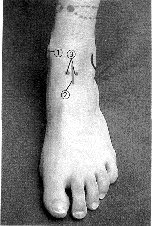
Landmarks: Dorsalis pedis a.2 Puncture sites: On both sides of dorsalis pedis a. Insertion of needle: Introduce the needle vertical to the skin directly beside the artery, up to slightly below it. Repeat on other side of a. Dosage: 2-3 ml 1 % lignocaine or prilocaine or 0,5% bupivacaine for each injection
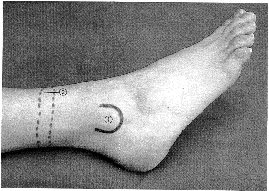
Landmarks: Lateral malleolus1, tibial edge, achilles tendon Insertion of needle: S. c. infiltration from the tibial edge to the achilles tendon about one hand's breadth above the lateral malleolus ^ S.c. infiltration from the tibial edge to the achilles tendon about one hand's breadth above the medial malleolus Dosage: 10-20 ml of 1% prilocaine or 0,25%-0,5% bupivacaine
Dosage for SVT : 1st 3-6 mg , if not effective within 1-2min 2nd 6 mg , if not effective within 1-2min 3rd 12 mg. ( Consider other drugs / methods if still not effective)
Method of administration
Rapid intravenous - over 1-2 seconds, via peripheral line
Site as proximal as possible to trunk (not in lower arm, hand, lower leg, or foot); follow each bolus with normal saline flush.
Follow each I.V. bolus of adenosine with normal saline flush.
In adults may be administered via a central line at lower doses (ie,initial dose: 3 mg).
Use
SVT including that associated with accessory bypass tracts (WPW), appropriate vagal maneuvers should be attempted prior to adenosine administration;
not effective in atrial flutter, atrial fibrillation, or ventricular tachycardia
2. Verapamil
Dosage for SVT : I.V.: 1st dose 2.5-5 mg (over 2 minutes); 2nd dose 5-10 mg (~0.15 mg/kg) may be given 15-30min after the initial dose if patient tolerates, but does not respond to initial dose; max total dose: 20 mg
Oral : 120 -480 mg/day in divided doses
Contraindications and Precautions:
Try to avoid using verapamil in the following condition;
heart failure, hypotension (systolic pressure <90 mm Hg) or cardiogenic shock; sick sinus syndrome (except in patients with a functioning artificial pacemaker); second- or third-degree AV block (except in patients with a functioning artificial pacemaker); accessory bypass tract (WPW, Lown-Ganong-Levine syndrome)
3. Amiodarone.
IV Amiodarone Loading : 300mg / 100cc D5% in ½ - 1hr, then Maintenance: 900mg/ 1 OD5% in 23 hrs or till arrhythmia is controlled (10-20mg/kg/day)
Or infusion @ 0.5 mg/min ( utilizing concentration of 1-6 mg/mL)
* A fast I.V.: 150 mg supplemental doses in 100 mL D5% over 10 minutes can be given in cases of breakthrough VF or VT
Contraindications and Precautions:
Severe liver disease, porphyria, thyroid dysfunction, Correct electrolyte disturbances, especially hypokalemia or hypomagnesemia, prior to use and throughout therapy. Prolonged QT syndromes.
4. Digoxin.
Dosage for Atrial Fibrilation
Initial: Total digitalizing dose: Give 1/2 of the total digitalizing dose (TDD) in the initial dose, then additional fraction in 4-8 hrs interval. Obtain ECG 6 hours after each dose to assess potential toxicity.
Oral: 0.75-1.5 mg I.V. or I.M.: 0.5-1 mg
Example; Digoxin 0.5mg stat followed by another 0.25mg x 2doses in 6 hrs interval
Daily maintenance dose: Give once daily Oral: 0.125-0.5 mg I.V. or I.M.: 0.1-0.4 mg
Contraindications and Precautions:
ventricular tachycardia or fibrillation; Wolff-Parkinson-White syndrome and atrial fibrillation concurrently, Correct hypokalemia and hypomagnesemia before initiating therapy, Use with caution in acute MI (within 6 months). Adjust doses in renal impairment and when verapamil or amiodarone are added to a patient on digoxin.
5. Lignocaine.
Dosage for Ventricular Tachycardia / fibrilation:
I.V.: 1-1.5 mg/kg bolus over 2-3 minutes; may repeat doses of 0.5-0.75 mg/kg in 5-10 minutes up to a total of 3 mg/kg;
Continuous infusion: 1-4 mg/minute
Infusion rates: 2 g/250 mL D5W (infusion pump should be used):
E.T. (loading dose only): 2-2.5 times the I.V. dose
Contraindications and Precautions:
Intravenous: Use cautiously in hepatic impairment, any degree of heart block, Wolff-Parkinson-White syndrome, CHF, marked hypoxia, severe respiratory depression, hypovolemia, history of malignant hyperthermia, or shock.
Increased ventricular rate may be seen when administered to a patient with atrial fibrillation. Correct any underlying causes of ventricular arrhythmias. Monitor closely for signs and symptoms of CNS toxicity. The elderly may be prone to increased CNS and cardiovascular side effects. Reduce dose in hepatic dysfunction and CHF.
Irregularly irregular rhythm No visible p waves or abnormal p Normal shape QRS
Treatment (Acute Fast Atrial Fibrillation)
- Oral or IV Digoxin - B Blockers - IV Amiodarone - Electrical Cardioversion
SUPRAVENTRICULAR TACHYCARDIA (SVT)
1. Regular rhythm 2. Narrow QRS complex tachycardia 3. Presence of P wave abnormalities - Deform p waves - No visible p wave ( p occur simultaneously with QRS which is compatible with reentry in the AV N) -P waves occurs after T ( compatible with reentry utilizing accesory AVN)
Treatment
- IV Adenosine - IV Verapamil - IV Amiodarone - Electrical Cardioversion
VENTRICULAR TACHYCARDIA (VT)
1. Broad QRS complex ( > 0.14 s) 2. Presence of atrioventricular dissociation 3. Bifid, upright QRS with a taller first peak in V1 4. Deep S wave in V6 5. A Concordant ( same polarity) QRS direction in all chest leads ( V1 - V6)
VT (Monomorphic)
VT (Polymorphic – Torsades Pointes)
VF
Treatment
- IV Lignocaine - IV Amiodarone - Electrical Cardoversion* Asynchronise electrical cardioversion is usually used in VF
BRADYARRHYTHMIAS
First Degree AV Block
Bradycardia, regular rhythm Prolongation of PR interval > 0.22s
Second Degree AV Block
(1) Mobitz type 1 ( Wenckebach )
progressive prolongation of PR interval until a P wave fails to conduct. Regularly irregular rhythm
(2) Mobitz type 2
PR interval of the conducted beat is constant with one p is not followed by a QRS complex.
Complete Heart Block
No relation between P and QRS complex Abnormal shaped QRS complex
Treatment - IV Atropine - IV Isoprenaline - Pacemaker – Temporary internal or external, Permenant
•Mechanism: rapid deceleration. •Trachea: blunt or penetrating. Usually just above or after carina. Typically fail phonation with stridor. •Esophagus: Fail NGT insertation. Pneumomediastinum / pneumothorax (left) •Mediastinal hemorrhage: most unrecognised clinically or radiologically. Indirect sign: mediastinal widening. •Aortic rupture: at the isthmus. Superior mediastinal widening.
PNEUMOMEDIASTINUM AND PNEUMOPERICARDIUM
•Result from: Pulmonary interstitial emphysema. Perforation esophagus, trachea or bronchus. From pneumothorax. From pneumoperitoneum.
PNEUMOMEDIASTINUM
•Vertical , translucent streaks, extend up to the neck. •Air collected beneath the diaphragm – continuous diaphragm sign.
MEDIASTINAL INJURY
•Pneumomediastinum. •Lung contusion. •Fail NGT insertion- suspicious of esophageal injury.
•Mediastinal emphysema and deviation of ETT. •Malalignment of ETT and trachea. •DDx: tracheal injury
•Fracture lower ribs. •No hemothorax – erect lateral view of the chest could detect small amount of blood in posterior costophrenic recess. •Anticipate solid organ injury.
•Fracture of 1st and 2nd ribs. •‘Apical cap’ – localised hemorrhage. •Look for any evidence of great vessel injury.
















 Saw- tooth appearance
Saw- tooth appearance
































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}